Introduction
During August of 2009 I traveled to the Netherlands for an Isolated Limb Perfusion procedure to treat a non-resectible sarcoma on my right forearm. Isolated Limb Perfusion is not a very well known cancer treatment in the United States and it's really hard to find easily digestible information about it. The goal of this document is to help fill that information gap (in a very small way) by describing my ILP experience. It's been quite an adventure and my hope is that it will help smooth the way for you or someone you know who is contemplating ILP.
Let's start by setting the scene. On April 1, 2009 an apparent rash on my right forearm was diagnosed as multi-focal Angiosarcoma. I began treatment at Memorial Sloan-Kettering Cancer Center in New York City. Surgery is usually the treatment of choice for Angiosarcoma. In my case it isn't an option because the tumor is too large and too diffuse. I started chemotherapy (Liposomal Doxorubicin) with the goal of shrinking the tumor to potentially undergo surgery in the future. After four months of chemo the surgeon at MSKCC examined me again. The tumor had responded to the chemo but it still wasn't resectible. Continuing with a longer chemo program wasn't a good option either. I was having serious skin toxicity problems from the Doxorubicin.
My options for long term local control of the disease were
becoming pretty limited. Amputation was beginning to loom large
as
the next step. During the follow up visit, my surgeon suggested
we
consider Isolated Limb Perfusion. If we agree to go that route he
urged
us to have the treatment
in Europe. He referred us to Dr. Alexander Eggermont, a surgeon
in the Netherlands who is an established expert in the field.
What is Isolated Limb Perfusion?
Isolated Limb Perfusion is, essentially, a chemotherapy procedure
for treating tumors of the arm or leg. Unlike regular systemic
chemo, ILP just applies the chemo to the limb. The limb is
isolated from the rest of the bloodstream with a tourniquet.
Since the circulatory system of the limb is isolated from the organs,
such
as the heart, very high doses of chemo can be used. The dose is
so high that the vascular system of the tumor is attacked and destroyed
in a single application. ILP is a one time procedure
(mostly). It is
not normally repeated like systemic chemotherapy.
At it's core ILP is a chemotherapy procedure, but in practice it is
a surgical procedure. It is performed in the operating theater
under general anesthesia
and takes 3 to 4 hours. There are three
basic phases to the surgery.
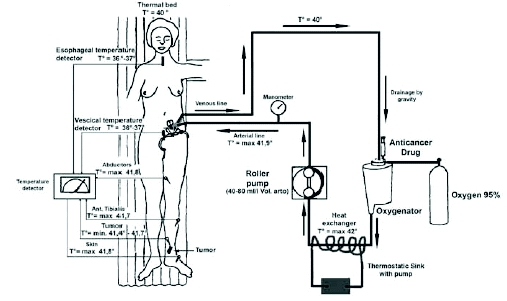
- Isolation of the Limb. The tourniquet is applied to the root of the limb (in my case, the shoulder). An incision is made to expose a major artery and vein that feed the limb. The two blood vessels are opened and connected to the input and output of a heart-lung bypass machine. The heart-lung bypass machine will circulate the chemo through the limb during the perfusion phase.
- Perfusion. The first step of the perfusion phase is to confirm that the tourniquet is not leaking. A radio-active tracer is introduced into the solution circulating through the limb. A gamma camera is positioned over the heart. If there is any leakage passsed the tourniquet there will be an increase in the radio-active counts measured at the heart. After the tourniquet has been confimed to not leak, the chemo is introduced to the circulating solution. The chemo is circulated though the limb for about 70 minutes.
- Clean Up. Clean saline solution is flushed through the limb to remove any residual chemo. The heart-lung machine is disconnected and the blood vessels are sealed. Finally, the incision that exposed the blood vessels is closed.
Why Travel to Europe for ILP?
This is a question we had to deal with often. The Americans wondered why we needed to go overseas for an "experimental" procedure. The Dutch assume that the very best medical care is available in the United States, so why are we coming from New York to a little out of the way clinic on the outskirts of Rotterdam for cancer treatment.First of all, ILP is not experimental. The technique has been around since the 1950s. Melanoma patients who are candidates for ILP can have the procedure performed in the US. The University of Pennsylvania, for example, has an experienced ILP program. So, if melanoma patients can get ILP in the US, why would a sarcoma parient travel to Europe? The answer lies in the chemo drugs. For melanoma, a single chemo drug (Melphalan) is used. The response rates using the single drug are quite good. However, sarcomas don't respond nearly as well to Melphalan alone. In the 1980s it was observed that sarcomas responded much better to a combination of Melphalan and TNF (Tumor Necrosis Factor). In the late 1990s a multi-center clinical trial was conducted in Europe for the treatment of sarcomas with Melphalan and TNF. Based on the results of this study the European regulatory agency approved the use of Melphalan and TNF for treating soft-tissue sarcomas of the extremities. However, a clinical trial of this type has not been conducted in the US and TNF has not been approved by the FDA. This means that ILP using TNF is not available in the US and one must travel to Europe where TNF has been approved since 1998.
The second question is why choose a not very well known clinic in the southern suburbs of Rotterdam? The answer is Dr. Alexander Eggermont. Dr. Eggermont has been one of the top researchers in refining and applying ILP and he practices at the Erasmus MC-Daniel den Hoed Cancer Center in Rotterdam. The clinic is relatively small and not very flashy, but the team of medical staff have as much (or more) experience with ILP than any other clinic in the world.
Initial Consultation
My wife and I met with Dr. Eggermont several days before the surgery. We found him to be a very charming man. He exudes both a sense of compassion as well as technical excellence. We didn't feel intimidated at all, it was a very comfortable meeting. After examining the tumor he spent some time explaining what to expect from the procedure. He described that he would make an incision along the muscle that forms the front edge of the armpit. The heart-lung bypass machine would connect to the main blood vessels leading to the arm through this incision.After discussing the details of the procedure, Dr. Eggermont asked what I did for a living. I work in Information Technology. This was significant for Dr. Eggermont. Since I spend much of my work day typing on a keyboard, he wanted to make sure the sense of touch in my fingertips wasn't affected. Initially he proposed putting a second tourniquet around my wrist. That would allow my arm to be perfused but would spare my hand from exposure to the drugs. If the hand and fingers are not perfused it reduces the chance of nerve damage that could impact the sense of touch. We discussed the red rash I had on the back of my hand. I couldn't be certain if this was Angiosarcoma or residual side effects of the Doxorubicin treatment. We agreed that it was too risky to isolate the hand from the perfusion. Dr. Eggermont still had a solution. He would place small individual tourniquets around the base of each of my fingers. Now, the hand can be perfused while still protecting the finger tips. Problem solved.
This initial meeting with Dr. Eggermont was on a Friday. Surgery was scheduled for the following Tuesday. His parting words were "there's nothing for you to do until Tuesday. Amsterdam is less than an hour away by train. It has fabulous museums and architecture. Go an enjoy yourselves".
Surgery
We stayed in the patient family house on-site so I didn't need to check in to the hospital until the morning of surgery. Surgery was scheduled for 8:00am so we reported to the surgical wing at 7:00am. I changed into a hospital gown, hopped into bed and in no time at all they wheeled me in to the surgical prep area. Two technicians began the process of hooking me up to IV drips, EKG and oxygen. The surgical team began to filter in and introduce themselves. There was the assistent surgeon, the anesthesiologist and shortly in bounded Dr. Eggermont. He shook my hand and said "it's your job to go to sleep now and my job is about to begin". The next think I know I'm waking up in the recover area. For me, the surgery was a piece of cake. They wheel me in, I go to sleep, I wake up and it's done. It was a little more stressful for my wife who had to wait in the waiting room for four hours before Dr. Eggermont came out to let her know that everything went smoothly.Post-surgical Recovery
This is the subject I knew least about. There was almost nothing that I could find by searching the web that described how long the recovery would take, what the side effects would be and how they would be treated. I'll describe my recovery, over time, but keep in mind I can only describe an arm perfusion. A leg perfusion may be quite different.Day 1
The first 24 hours of recovery is in the intensive care unit. The stay in intensive care is precautionary just to watch for any immediate side effects from the TNF. I didn't experience any side effects. I did have one unusual response that had the doctors rather intrigued. The finger tips of my right hand became very cold as if they were getting no blood circulation. Later, they warmed up to a normal temperature and then they become very cold again. The doctors had never seen this cycling of body temperature. The ICU staff called in Dr. Eggermont. He didn't seem too concerned. He felt it was a vaso-constriction response to the perfusion and he expected it to settle down within 24 hours or so. The fingertips stopped cycling by the end of the first day just as Dr. Eggermont predicted.
Week 1
Dr. Eggermont's team have learned from experience that a patient's reactions to the perfusion doesn't materialize immediately. The reaction will increase with time and peak around day 7. In other words you won't begin to feel better during the first week, you will actually feel progressively worse. The medical team will watch closely during that first week for any signs of serious reactions. They have learned that serious reactions usually show up within that first week. For that reason they will not clear you to fly home during the first week. They want you close at hand so they can immediately treat a serious reaction.
The normal (non-serious) reactions include general redness of the limb, some swelling and aching of the muscles. The muscle aches are similar to the achiness you feel when you have a case of the flu. The thick muscle on the top side of my forearm, just below the elbow, was rather more painful. One of the surgeons explained that they embed two temperature probes into that thick muscle during the perfusion, which explains the extra discomfort in that area.
After the first 24 hours in intensive care you are moved to a regular hospital room on the surgical wing. These are shared rooms, and unlike American hospitals, these rooms are coed. Almost immediately after they have you settled into the hostpital room you are encouraged to put your street clothes on and begin to walk around. The nurses put me in an old fashioned sling to support my arm while I was walking around.
I stayed in the hospital room for about two days and then I was released back to the Family House on the third day. We had several days to kill before our day 7 follow up visit with Dr. Eggermont. We used those days to take some not-to-strenuous sight seeing trips around Rotterdam. These included a boat trip to see windmills, another boat tour of the sea port and a tram trip into the center of the city in search of Dutch pancakes.
The follow up visit with Dr. Eggermont went very well. He was very pleased that no serious side effects had materialized. As a result, he cleared us to fly back home. We asked him what to expect for the next several months. Specifically, we asked "how long will it take before we know how well the perfusion has worked?" He actually answered a slightly different question when he said "it will take about 6 weeks before the normal tissue settles down enough to do an evaluation".
Week 2
The day we flew out of Rotterdam I started to develop a bright red rash on the back of hand and top of my forearm. I was concerned that Dr. Eggermont didn't see it. I already had a followup visit with my medical oncologist (Dr. Maki) on the calendar for the day after we arrived home. We decided to keep that appointment even though it was much too soon. Dr. Maki referred me to a rehabillitation specialist at MSKCC (Dr. Stubblefield). The thinking being that Dr. Stubblefield could use massage techniques to help reduce the edema. When we saw Dr. Stubblefield he decided not to do anything to treat the edema. The swelling was going down on its own and he didn't want to risk spreading the tumor. He did prescribe Atarax to relieve the itching of the red rash on the back of my hand. He also prescribed physical therapy to regain the strength and range of motion in my right arm.
Week 4
After about two weeks the red rash on the back of my hand had mostly gone. The physical therapy was already showing a marked improvement in the range of motion of my shoulder. The elbow and wrist were going to take longer. One thing I didn't expect was that the therapist would spend a few minutes each session massaging the surgical scar along the front edge of my armpit. Initially it looked really thick and ropey and after a couple of weeks of massage it was down to a thin pink line.
Week 6
As Dr. Eggermont had predicted, most of the initial ILP reactions; the redness, swelling and aching muscles had disappeared by about week 6. The distinct red spots of the Angiosarcoma were becoming less red and less well defined. They had changed from red spots to pink smudges. A number of the skin irritation problems still persisted. At times the surface of the skin would itch, at other times it would burn and sometimes it would feel bruised or numb.
Week 8-9
It may have been happening earlier, but I didn't notice the hair loss on the back of my hand and forearm until about week eight. This was another side effect that Dr. Eggermont predicted. By about week 8-9 I started to develop dense tissue in the bend of by elbow. This dense tissue could be quite painful at times.
Week 10
Week 10 was the week of the big checkup. This would be the first real evaluation after the inital ILP reactions had subsided. Dr. Maki (medical oncologist) was very pleased with how the arm looked. I put him on the spot and asked him to evaluate my response to the ILP. He described it as "pretty close to a complete response". He prescribed no further treatment and scheduled me to have my chemo port removed. The on-going regemine will be a CT scan and follow up visit every four months and to watch vigilantly.
We had scheduled a follow up visit with Dr. Stubblefield on the same day. Dr. Stubblefield described my skin irritation problems as classic symptoms of Neuropathy. He suggested I try Lyrica to help relieve the symptoms. The continuing weakness in my hand and thumb was consistent with Median Mononeuropathy (aka Carpal Tunnel Syndrome). In my case, Dr. Stubblefield felt the pressure on the Median nerve was coming from the scar tissue in the bend of my elbow rather than the wrist where it normally occurrs. He recommended additional soft tissue massage during physical therapy to help break up the scar tissue around the elbow.
Week 15
After 13 weeks of physical therapy my therapist said "enough". The strength and range of motion had mostly returned. The thumb and wrist were still a little stiff, but a huge improvement over the starting point. The scar tissue around my elbow had also become more supple. Was it reaction to the ILP alone that dictated so much physical therapy? I don't think so. I think the range of shoulder motion, pain and weakness in the palm of my hand, and weakness in my thumb could be attributed directly to the ILP. The general weakness in the elbow, wrist and forearm may well have resulted from favoring the right arm during the first four months following diagnosis. During that period I found that if I excercised the arm too much it would swell. The swelling was uncomfortable so I often switched to using my left hand. Favoring the right arm led to muscle atrophy and that took quite some time to recover.
You're going to Rotterdam for ILP, what next?
Your physician has recommended ILP and has referred you to Erasmus
MC-Daniel den
Hoed Cancer Center in Rotterdam. What do you do now? We
found the logistics of getting there and living there to be quite an
adventure. In this section I'll point some of the things we
learned along the way. Being aware of some of these realities up
front will hopefully make your journey a little easier.
Amsterdam is your most likely port of entry from the US. We
flew direct from Newark, NJ to Amsterdam's Shiphol airport.
Find out when your first hospital appointment is scheduled and then
plan your flight to arrive at least a day ahead of time. Book a
flight that arrives early in the morning. That will give you
plenty of time to find your way to Rotterdam and get checked in to your
accommodations. The trip will be a little more stressful than
you're used to so don't add to the stress by cutting your time too
short.
Currency Exchange
Before you leave exchange plenty of cash. You'll need a lot
more Euros than you might expect. We hoped to pay as much as
possible with credit cards. That turned out to be a big
mistake. For starters, the Family House only takes cash so you'll
need enough for two weeks accommodation. The second problem is
that American style credits cards don't work in a lot of places.
What I mean by an "American style" card is one where the merchant
prints out a paper receipt and you sign the receipt with a pen.
The Europeans have moved beyond wet ink signatures and now use a PIN
system. Instead of signing a reciept you enter a PIN on a
keypad. It's much like a US debit card. I had a Visa debit
card with me and I tried to use it a few times. I think it worked
once. You will be able to use your American style credit card at
places that see a lot of tourist traffic like the museums. We had
about a 50% success rate in restuarants.
Travel to Rotterdam
Rotterdam is about 80km southwest of Amsterdam. Train is by far your best option for traveling to Rotterdam. It takes about 50 minutes and costs about €12 per person. We were told that a taxi would cost about €180. You can board a train directly from Amsterdam's Shiphol airport. There is a ground transportation concourse area just before you exit the airport to the street. There is a very handy information booth there and ticket counters for purchasing train tickets. Purchase tickets to Rotterdam Centraal station. I'd recommend you pay cash for the tickets to avoid confusion. Ask the ticket agent for the time and track number of the next train to Rotterdam. The train platforms are one level below the ground transportation concourse. There are escalators (and elevators) in the concourse that take you down to the various tracks. Look for the one that leads to your track.
 Each
of the stops the train makes will be listed on an overhead signboard on
each track. Make sure you see Rotterdam
Centraal listed. It will be about 4 stops from Amsterdam
Shipol. There's not a lot of storage space for luggage on the
trains. If the train is not too full you can set you bags on the
seat next to you. If the train is full you need to stuff then
under your seat or maybe stack them in the vestibule at the end of the
car. Once you've taken your seat, sit back and relax and enjoy
the dutch countryside for an hour.
Each
of the stops the train makes will be listed on an overhead signboard on
each track. Make sure you see Rotterdam
Centraal listed. It will be about 4 stops from Amsterdam
Shipol. There's not a lot of storage space for luggage on the
trains. If the train is not too full you can set you bags on the
seat next to you. If the train is full you need to stuff then
under your seat or maybe stack them in the vestibule at the end of the
car. Once you've taken your seat, sit back and relax and enjoy
the dutch countryside for an hour.
Getting to the Hospital
Once you arrive at Rotterdam Central your next task is to find your way to the hospital. The Daniel den Hoed Cancer Center is a branch of the main Erasmus Medical Center. It is not in the center of the city. It is about 6km to the south in Rotterdam-Zuid (South Rotterdam). You have a couple of different options for making your way to the hospital.Taxi
We did not take a taxi. There was another American couple who
arrived while we were in Rotterdam. By the time they reached
Rotterdam station they were exhausted so they opted for
a taxi to avoid dealing with local public transportation. I don't know
how much it cost. The one problem they encountered is that the
driver initially took them to the main Erasmus MC is the center of the
city. They hadn't made it clear enough that they wanted to go to
the Daniel den
Hoed Cancer Center.
Tram
 We opted to take the tram. Rotterdam has an
extensive tram network and we used it quite a bit. The tram is an
above ground light rail system. Don't confuse it with the Metro
which is their underground subway.
We opted to take the tram. Rotterdam has an
extensive tram network and we used it quite a bit. The tram is an
above ground light rail system. Don't confuse it with the Metro
which is their underground subway.
When you arrive at Rotterdam Central station you descend stairs from the platform into a tunnel. We could not find any escalators or elevators so we had to drag our luggage down the stairs. There are no signs in the tunnel to tell you which way to go. You need to go to the end of the tunnel where you see lots of yellow signs, yellow ticket machines and the yellow Metro station. If you don't see these, try the other end of the tunnel. Each time we arrived at Rotterdam Central we turned right when we entered the tunnel, although, that really depends on which stairs you choose to descend from the platform. When you exit the tunnel, follow the signs to the tram.
 At the
tram stop purchase tickets to Sandelingplein (pronounced
SUNDer-ling-PLANE). The tickets will cost about €3 per
person. You can also buy tickets from the conductor on the
tram. The tram stop at Rotterdam Central has several
platforms. There are electronic overhead signs on each platform
that display the tram number and final station for the next arriving
tram. Look for tram 25
to Carnisselande.
Your stop, Sandelingplein, is about 12-13 stops from Rotterdam
Central. Each stop is displayed on an electronic sign on the
ceiling of the tram and announced by a recorded voice. You get
off when you see Sandelingplein
displayed and the announcement sounds like SUNDer-ling-PLANE.
At the
tram stop purchase tickets to Sandelingplein (pronounced
SUNDer-ling-PLANE). The tickets will cost about €3 per
person. You can also buy tickets from the conductor on the
tram. The tram stop at Rotterdam Central has several
platforms. There are electronic overhead signs on each platform
that display the tram number and final station for the next arriving
tram. Look for tram 25
to Carnisselande.
Your stop, Sandelingplein, is about 12-13 stops from Rotterdam
Central. Each stop is displayed on an electronic sign on the
ceiling of the tram and announced by a recorded voice. You get
off when you see Sandelingplein
displayed and the announcement sounds like SUNDer-ling-PLANE.
When you get off you'll be deposited on a very non-descript suburban
street (Groene Hilledijk) with no indication of which way to go.
Walk about 150 yards along the street, in the
same direction the tram is traveling. When you come to the
hospital you'll see a sign to Familiehuis.
Follow the sign up the drive. The entrance to the Familiy House
is on the opposite side to the street. One of the volunteers will
let you in and bring you into the office. You've had a very
trying day so take the opportunity to relax for a little bit before the
staff gives you an orientation to the facility.
Accommodation
I have mentioned the Family House several times. Now it's time
to explain what it is. It is a guest house situated on the
hospital site. It's purpose is to provide accommodation for the
family members of patients undergoing prolonged treatment. The
Family House volunteers try to avoid this comparison, but it's a little
like the Ronald McDonald houses in the US. However, the Family
House is not oriented toward children undergoing care and it doesn't
have any corporate sponsorship. It operates strictly on private
donations and a dedicated staff of about 50 volunteers. The
Family House web site is http://www.familiehuis.nl/. It is all in
Dutch and it doesn't have an on-line English version. You can get
Google to translate it for you by pasting the URL into the Google
search field and clicking Search. Then click the [Translate this
page] link of the first search result.
 The Family
House is a cylidrical building with thirteen guest rooms arranged on
two floors. There is a central stairwell and the rooms on each
floor are arranged in quadrants like slices of a pizza. The guest
rooms are small with two twin beds, a small bathroom, a desk, a coffee
table, a TV and an electric fan. There is no air
conditioning. We hit an unusually warm spell during our stay so
that little electric fan became our best friend.
The Family
House is a cylidrical building with thirteen guest rooms arranged on
two floors. There is a central stairwell and the rooms on each
floor are arranged in quadrants like slices of a pizza. The guest
rooms are small with two twin beds, a small bathroom, a desk, a coffee
table, a TV and an electric fan. There is no air
conditioning. We hit an unusually warm spell during our stay so
that little electric fan became our best friend.
The Family House also includes:
- A couple of common living rooms with a TV, DVD player and two
computers guests can share. There is wireless internet available
in the building.
- A common kitchen for preparing meals.
- A common dining area right next to the kitchen.
- A common laundry in the basement with coin operated washes
and dryers.
- There are a couple of bicycles you can borrow and a couple of
little grocery carts you can borrow if you're walking to the grocery
store.
The Family House is not a hotel. Guests are expected to help
keep the common areas clean as they do their guest rooms.
Dutch residents with Dutch insurance pay about €25 per day to stay
at the Family House. You'll pay about €52 per day because you
don't have Dutch insurance. Remember, the Family House only takes
cash.
Meals
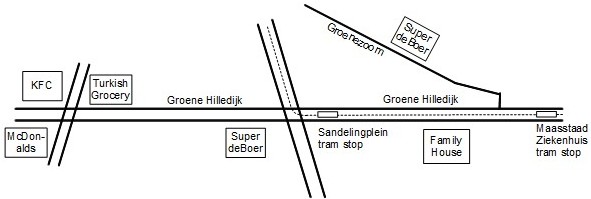
The area immediately around Daniel den Hoed Cancer Center is a very blue collar, Turkish neighborhood. There is a commercial center on Groene Hilledijk with lots of shops. Turn left out of the Family House onto Groene Hilledijk and walk past the Sandelingplein tram stop. You will find a number of snack bars, pastry shops and bars. However, there are very few (if any) sit down restaurants along this strip. With very few restaurants in the immediate area, you'll need to look for alternatives for meals.
Hospital Cafeteria
The hospital staff cafeteria is available to the Family House residents. The cafeteria serves breakfast and lunch five days per week. Breakfast is available from 9:15am to 10:30am and lunch is served from 12:00pm to 2:00pm. The cafeteria is small and the selection is limited.
Family House Kitchen
With the cafeteria closed on evenings and weekends you will have to make use of the Family House kitchen. It's really a very nice facility. Each room is assigned a small refrigerator and a kitchen cabinet. There are four electric stoves that are shared by the guests each with a set of pots and pans. Silverware and dishes are available from a common cabinet. There are two dishwashers for the silverware and dishes. You are responsible for washing your pots and pans by hand. Next to the cooking area there is a dining area with a number of separate tables and chairs.
Grocery Stores
You'll need the ingredients for all the meals you prepare in the kitchen. There are several grocery stores within walking distance of the Family House. The closest is a Super de Boer on Groene Hilledijk just beyond the Sandelingplein tram stop. A slightly larger (and more turkish) grocery store is further along Groene Hilledijk on the corner across from Kentucky Fried Chicken. A second Super de Boer is located on Groenezoom. We preferred this one of the three. It's brighter and a little less hectic.
We always paid cash at the grocery stores. Even though you see the locals paying with plastic, they would not take Visa.
Shopping Mall
There is shopping mall within a longish walk (about 20 min) of the Family House. One of the other guests at the Family House told us about it. We would never have found it on our own.
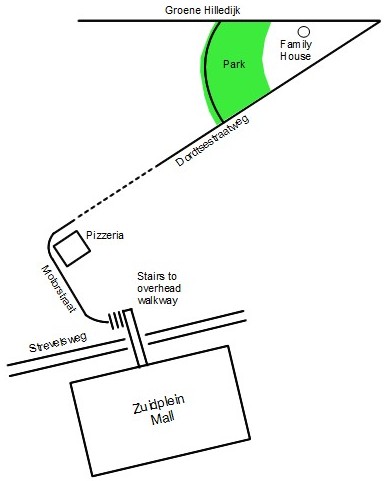 Turn left out of the Family House onto Groene Hilledijk. Turn
left into the park and walk through the park to the road at the far
end. Turn right onto that road (Dordtsestraatweg). Follow this road
until it bends around to the left at a pizzeria. Soon after rounding
the bend you will see a large set of steps. Take the steps up to the
walkway which crosses the road into the mall.
Turn left out of the Family House onto Groene Hilledijk. Turn
left into the park and walk through the park to the road at the far
end. Turn right onto that road (Dordtsestraatweg). Follow this road
until it bends around to the left at a pizzeria. Soon after rounding
the bend you will see a large set of steps. Take the steps up to the
walkway which crosses the road into the mall.